


Blood Transfusion Management
Risks and Costs of Red Blood Cell Transfusions
Red blood cell (RBC) transfusion is one of the most frequent procedures performed in US hospitals, with one in ten inpatients receiving one or more blood units.1 While blood loss during surgery is a known risk factor, RBC transfusion overuse can increase patient risk and cost of care. Meta-analysis of pooled results from multiple observational studies, each of which adjusts for risks between patients, shows that patients receiving RBC transfusions have an 88% higher mortality, 69% higher infection rate, and 250% higher rate of acute respiratory distress syndrome (ARDS).2 Multiple randomized controlled trials indicate that restrictive transfusion practices—those in which significantly lower hemoglobin triggers are used to determine need for transfusion—are safe.3 In addition, the cost of each RBC unit is estimated between $522 and $1,183 per unit, without including morbidity-associated costs.4 Beyond the cost of transfusion, each RBC unit transfused is associated with increased cost of care and transfusions that occur at higher hemoglobin levels increase the cost of care more than those given at lower hemoglobin levels.5
With the growing recognition of the need to reduce transfusions, noninvasive and continuous hemoglobin (SpHb) can be a key tool to help overcome the limitations of existing approaches.

The Growing Recognition of the Need to Reduce Transfusions
Many transfusions are unnecessary. A systematic, expert review of 494 studies for positive impact on health outcome showed that 59% of RBC transfusions are "inappropriate."6 Given the risks and costs of RBC transfusions, there is a growing recognition of the need to implement strategies to reduce RBC transfusions. The Joint Commission has introduced Patient Blood Management Measures that encourage hospitals to evaluate appropriateness of transfusions as a continuous quality indicator.7 The American Medical Association and The Joint Commission also recently identified RBC transfusions as one of the top five overused procedures in medicine, defining overuse as "circumstances where the likelihood of benefit is negligible or zero, and the patient is exposed to the risk of harm."8
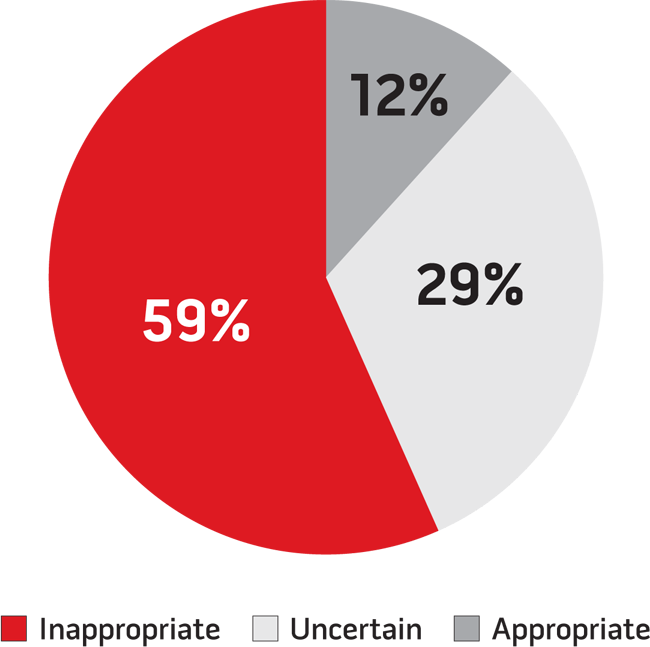
Figure.
494 studies were evaluated by an expert panel in a systematic method to assess appropriateness of RBC transfusion, revealing a significant opportunity to reduce unnecessary transfusions.6
Limitations with Existing Approaches to Assess Transfusion Need
Hemoglobin levels are used as a primary indicator for RBC transfusion, but laboratory measurements are only available intermittently and results can be delayed in the period between blood draw and laboratory analysis. This time gap of information can lead to sub-optimal transfusion decisions.9
The most universally available information about whether a transfusion is needed during surgery is estimated blood loss, which is often overstated. Visible blood and fluid loss appears to tell one how much blood has been lost, but in a recent study at Duke University, anesthesiologists estimated blood loss at 40% more than it actually was.10 The implication is that the need for transfusion may appear to exist, when in fact it does not.
How SpHb Monitoring Helps with Transfusion Decisions
Masimo's solution provides hemoglobin both noninvasively and continuously. The noninvasive aspect makes the technology easy to apply to the patient, and the continuous aspect assists in better decision making. While SpHb monitoring is not intended to replace blood draws, it identifies significant changes in hemoglobin and lack of significant changes in hemoglobin between invasive blood sampling and laboratory analysis.11
Continuous hemoglobin means clinicians can determine the directional trend of hemoglobin—whether it is stable, rising, or falling. This can help avoid unnecessary transfusions when the SpHb trend is stable and the clinician may otherwise perceive hemoglobin is dropping, or when the SpHb trend is rising and the clinician may otherwise perceive it is not rising fast enough. Inside and outside the operating room, a dropping SpHb trend may also allow clinicians to identify internal bleeding and permit earlier interventions.
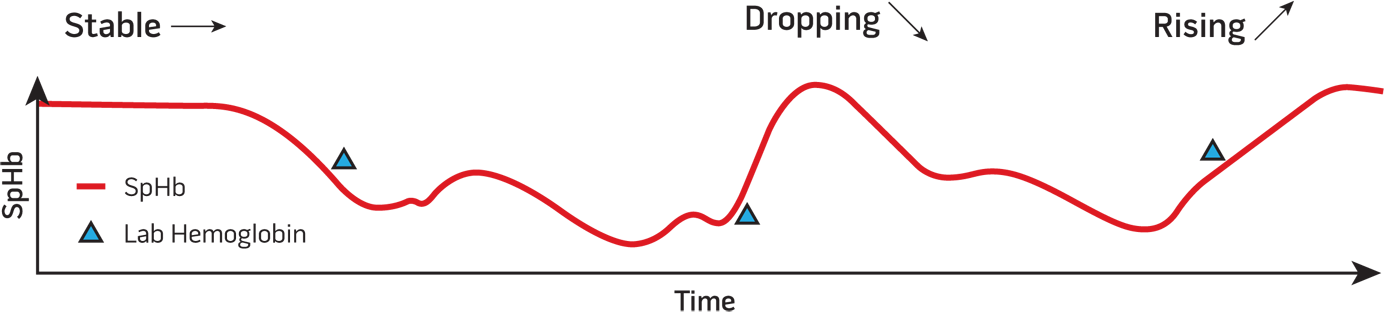
Figure.
Continuous hemoglobin trending between invasive blood sampling provides a real-time indication of whether hemoglobin is stable when it may appear to be dropping, rising when it may not appear to be rising, or dropping when it appears to be stable.
Clinical Evidence that SpHb Monitoring Helps Reduce Transfusions
There are now two studies showing that SpHb monitoring helps clinicians reduce RBC transfusions.
SpHb monitoring has been shown in a randomized controlled trial in low blood loss surgery (orthopedic surgery) to reduce the frequency of intraoperative blood transfusions by 87% (from 4.5% to 0.6%) and the average number of RBC units transfused by 90% (from 0.1 to 0.01 units per patient).12
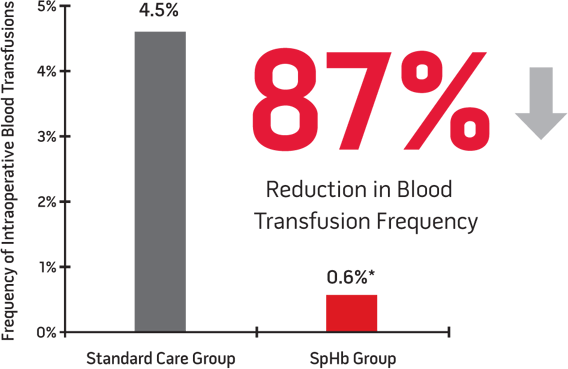
Figure.
Prospective cohort study in 327 orthopedic patients.
p<0.003 vs. Standard Care Group.
SpHb monitoring has also been shown in a prospective cohort study in high blood loss surgery (neurosurgery) to reduce the percent of patients receiving three or more RBC units from 73% to 32% and reduce the average number of RBC units transfused by 47% (from 1.9 to 1.0 units per patient).12 In this study, the researchers also showed that patients who needed RBC units received them sooner by 41 minutes on average.
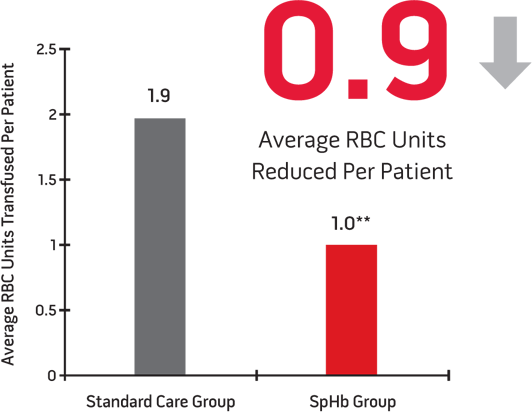
Figure.
Prospective cohort study in 106 neurosurgery patients.
p<0.001 vs. Standard Care Group.
SpHb also helps clinicians decrease the time to transfusion, when a transfusion is truly indicated13
![]()
Figure.
Prospective cohort study in 106 neurosurgery patients.
** p<0.001 vs Standard Care Group
 |
Projected Cost Savings from SpHb Monitoring to Reduce Transfusions
To project the potential savings from SpHb monitoring, the range of published cost estimates for RBC transfusions ($522 to $1,183) can be multiplied by the expected reduction in RBC transfusions per patient.4 In lower blood loss surgery, the 0.09 lower RBC units per patient with SpHb monitoring is projected to reduce RBC costs by $47 to $106 per patient monitored.12 In higher blood loss surgery, the 0.90 lower RBC units per patient with SpHb monitoring is projected to reduce RBC costs by $470 to $1,065 per patient monitored.13 These estimates do not take into account the expense of SpHb monitors or sensors, or the other costs associated with over transfusion or delayed care.
| Potential Blood Cost Savings Per Patient with SpHb Monitoring4 |
||
| Range of RBC Transfusion Cost Estimates |
Lower Blood Loss Surgery12 |
Higher Blood Loss Surgery13 |
| $522 | $47 | $470 |
| $1,183 | $106 | $1,065 |
REFERENCES
- 1 AHRQ. Inpatient Sample. 1997-2007.
- 2 Marik PE.et.al. Crit Care Med. 2008;36(9):2667-74.
- 3 Carson et al. Cochrane Database Syst Rev. 2012 Apr 18;4:CD002042.
- 4 Shander A et al. Transfusion. 2010;50(4):753-765.
- 5 Murphy G J et al. Circulation. 2007;116:2544-2552.
- 6 Shander et al. TransMed Rev. 2011. 232-246.
- 7 Joint Commission Perspectives. The Joint Commission Continues to Study Overuse Issues. Volume 32, Number 5, 2012: 4-8(5).
- 8 http://www.jointcommission.org/patient_blood_management_performance_measures_project/
- 9 Friedman MT et al. Arch Pathol Lab Med. 2006 Apr;130(4):474-9. 5 Hill SJ et al. ASA. 2011 (abstract).
- 10 Hill SJ et all. ASA. 2011 (abstract).
- 11 Frasca D et al. Crit Care Med. 39(10); 2011; 2277-2282.
- 12 Ehrenfeld JM et al. ASA. 2010. LB05. (abstract)
- 13 Awada W.F.N., Maher F. Proceeding of the Society for Technology in Anesthesia Annual Meeting, 2013: p 51.